High B12 Levels After Injection Pernicious Anemia: Definition, Symptoms, Causes & Treatment
Introduction
If you’ve ever had bloodwork show high b12 levels after injection and wondered whether that’s automatically “good news,” you’re not alone. In my clinical work, I’ve seen patients (and even clinicians) misread lab patterns—then miss the real issue behind abnormal B12 balance. This article breaks down pernicious anemia: what it is, the symptoms that actually matter, why it happens, and how treatment is managed long-term.
You’ll learn how “high B12 after injection” can fit into a bigger picture, what to watch for during therapy, and what diagnostics help confirm pernicious anemia so treatment targets the root cause—not just the lab number.
What Is Pernicious Anemia?
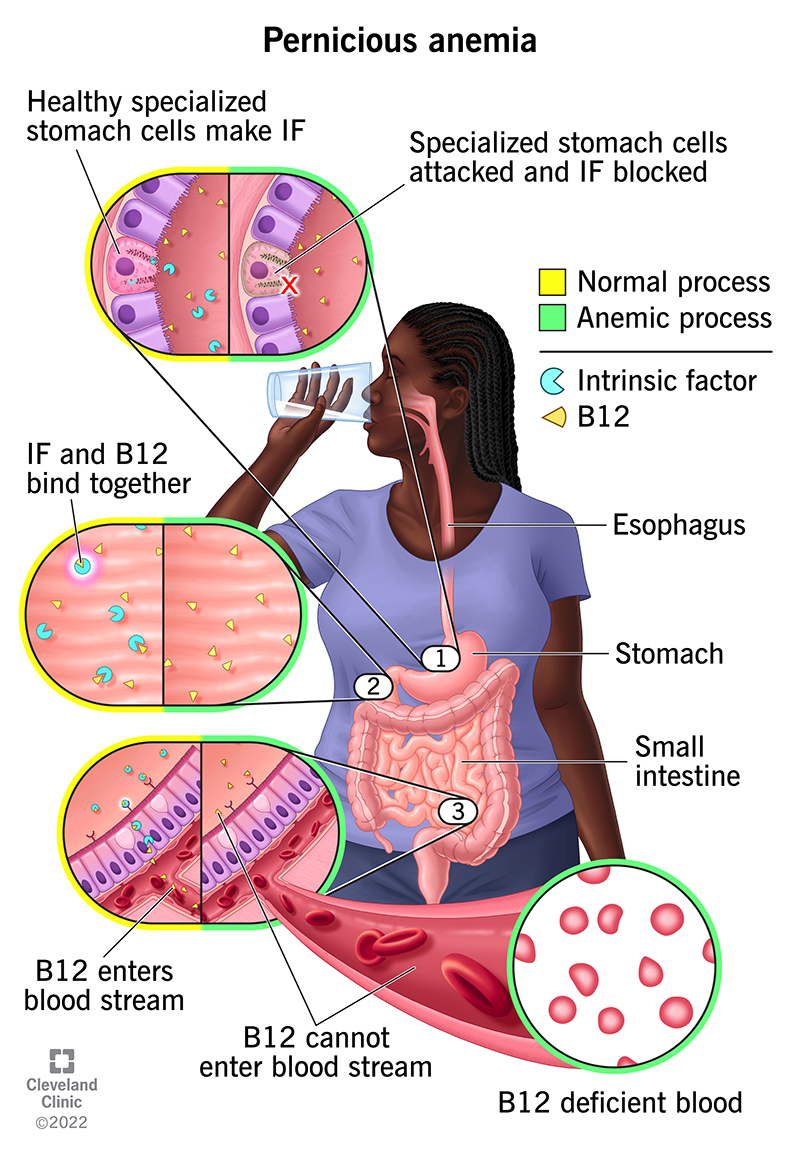
Pernicious anemia is a type of megaloblastic anemia caused by impaired absorption of vitamin B12 in the gut. The classic mechanism involves autoimmune damage to stomach cells that produce intrinsic factor—a protein required to absorb B12 in the small intestine.
Without intrinsic factor, oral B12 often fails to correct deficiency reliably, which is why treatment frequently involves vitamin B12 injections (or, in some cases, high-dose oral therapy under specific conditions). Over time, inadequate B12 absorption leads to impaired DNA synthesis in red blood cells and—importantly—neurologic complications if not treated promptly.
Symptoms of Pernicious Anemia (Including the Stuff People Miss)
Symptoms tend to develop gradually. In my hands-on experience, patients often report fatigue first, then realize they also have neurologic or cognitive symptoms that don’t “feel” like anemia. Below are the patterns clinicians typically look for.
Common anemia-related symptoms
- Fatigue, reduced exercise tolerance
- Shortness of breath with exertion
- Pale skin
- Dizziness or lightheadedness
- Headaches
Neurologic symptoms (can occur even before anemia is obvious)
- Numbness, tingling, burning sensations (especially in hands/feet)
- Balance problems or unsteady walking
- Memory or concentration difficulties
- Muscle weakness
Red blood cell and mouth/throat signs
- Glossitis (inflamed, sore tongue) and mouth discomfort
- Cracks at corners of the mouth
- Unexplained nausea or appetite changes
Key point: If neurologic symptoms are present, clinicians generally aim to start appropriate B12 replacement quickly—because delays can reduce the chance of full neurologic recovery.
Causes and Risk Factors
The underlying cause of pernicious anemia is autoimmune impairment of B12 absorption. But several related factors influence who gets diagnosed and how the disease progresses.
Autoimmune intrinsic factor deficiency
In pernicious anemia, the immune system targets components involved in intrinsic factor production and/or stomach function. This reduces B12 absorption even if dietary intake is adequate.
Associated autoimmune conditions
In many patients, pernicious anemia clusters with other autoimmune disorders. Common associations include:
- Autoimmune thyroid disease (e.g., Hashimoto’s or Graves’)
- Type 1 diabetes
- Other autoimmune gastrointestinal conditions
Why “normal B12 intake” doesn’t prevent it
I’ve counseled patients who were taking multivitamins or eating B12-rich diets yet still developed deficiency. That’s because the problem isn’t usually intake—it’s absorption. Without intrinsic factor, the system can’t reliably capture B12 from the gut.
How Pernicious Anemia Is Diagnosed
Diagnosis is a combination of clinical evaluation and lab testing. The goal is to confirm B12 deficiency and identify the cause as autoimmune/pernicious rather than another etiology.
Initial bloodwork clinicians commonly review
- CBC (often shows anemia with large red blood cells—macrocytosis)
- Serum vitamin B12 (may be low initially)
- Methylmalonic acid (MMA) and/or homocysteine (often elevated in true functional B12 deficiency)
Tests that support pernicious anemia specifically
- Intrinsic factor antibodies (more specific)
- Parietal cell antibodies (supportive)
- Sometimes reticulocyte count to assess marrow response after treatment starts
Clinical logic: A low B12 with elevated MMA supports deficiency. Antibodies help tie the deficiency to pernicious anemia rather than medication effects, dietary insufficiency, or other malabsorption syndromes.
Does Pernicious Anemia Treatment Cause High B12 After Injection?
Yes—often. When patients receive vitamin B12 injections, serum B12 can rise substantially. That’s not inherently harmful, and it can simply reflect absorption into the bloodstream from the injected dose.
However, I’ve learned the hard way that “high b12 levels after injection” shouldn’t be interpreted in isolation. The clinically meaningful outcome is whether the body corrects the deficiency and whether neurologic symptoms stabilize or improve.
What high B12 after injection can mean
- Expected response: After injections, the serum level can overshoot because the dose is delivered directly.
- Functional correction still matters: Even if serum B12 rises, MMA/homocysteine (and symptoms) help confirm the deficiency pathway has normalized.
- Timing affects interpretation: A high B12 measured shortly after an injection may not represent the trough level later in the dosing cycle.
Practical takeaway
If your clinician is tracking treatment, they typically focus on: symptom trajectory, CBC recovery, and (when needed) markers like MMA—rather than reacting to a single serum value.
Treatment Options for Pernicious Anemia
Treatment centers on replacing vitamin B12 and addressing the underlying absorption failure. Many patients require long-term therapy because the autoimmune cause persists.
Vitamin B12 injections
Injections are a common approach because they bypass the need for intrinsic factor in the gut. In my experience, this method provides reliable correction, especially for patients with severe deficiency or neurologic involvement.
High-dose oral vitamin B12 (selected cases)
Some patients can use high-dose oral B12 because a small percentage can be absorbed via intrinsic factor–independent pathways (passive diffusion). Whether this is appropriate depends on severity, response, adherence, and clinician judgment.
What monitoring usually looks like
- Symptom improvement: fatigue often improves first; neurologic recovery may take longer.
- Hematologic response: CBC parameters and reticulocyte response can reflect recovery of marrow function.
- Functional markers (when needed): MMA/homocysteine may be checked to confirm biochemical correction.
- Dose schedule adjustments: regimens can include an initial phase followed by maintenance.
Limitations and realistic expectations
Even with appropriate treatment, full neurologic recovery isn’t guaranteed—especially if symptoms have been present for a long time before therapy begins. Also, serum B12 can become high after injection; the goal is not merely “lowering” B12, but restoring function and preventing relapse.
Common Questions Patients Ask During Treatment
When pernicious anemia is suspected or confirmed, patients often want clarity on what to expect after starting therapy—particularly around lab results and symptoms.
- “Why do my B12 levels look high now?” (Often expected after injection and timing matters.)
- “Will I need treatment forever?” (Many do, due to the persistent autoimmune cause.)
- “What if my symptoms don’t improve quickly?” (Neurologic recovery can lag; clinicians may reassess dosing and confirm diagnosis.)
FAQ
Why are my B12 levels high after injection?
Vitamin B12 injections deliver B12 directly into the body, so serum levels commonly rise—especially if your blood test was done soon after a dose. Clinicians interpret this alongside symptom improvement and, when appropriate, functional markers like MMA rather than focusing on serum B12 alone.
How can I tell if it’s truly pernicious anemia and not another cause of B12 deficiency?
Diagnosis usually combines evidence of B12 deficiency (often with elevated MMA/homocysteine) and tests for pernicious anemia such as intrinsic factor antibodies. A comprehensive evaluation also considers other causes of macrocytosis and malabsorption.
Will high B12 after treatment cause problems?
High serum B12 after injection is frequently an expected treatment effect. The key is how you’re responding clinically and biochemically. Your clinician may adjust monitoring strategy based on symptoms, blood counts, and (if needed) functional markers—rather than stopping therapy due to a single elevated serum value.
Conclusion
Pernicious anemia is an autoimmune condition that impairs intrinsic factor and prevents reliable B12 absorption, leading to anemia and potentially serious neurologic symptoms. Treatment often involves vitamin B12 injections, and that can produce high b12 levels after injection—which is usually expected. The most important outcomes are symptom recovery, hematologic response, and confirmation of functional correction (not just one lab number).
Next step: If you have confirmed or suspected pernicious anemia, ask your clinician what monitoring plan they’re using (symptoms, CBC, and whether MMA/homocysteine are needed) and how they interpret serum B12 results relative to your injection timing.
Discussion