Ghk Cu Injection Sites GHK-Cu Peptide Therapy: The Definitive Clinical Guide to Gene Modulation, Protocols, and Efficacy
If you’ve ever tried to make sense of GHK-Cu peptide therapy—especially how gene modulation is supposed to translate into real outcomes—you’ve probably hit the same wall I did: information is scattered, protocols vary widely, and the most practical details (like ghk cu injection sites, needle placement logic, and what to expect from day to day) are rarely explained clearly.
In this clinical-style guide, I’ll walk you through the underlying science in plain language, the most important protocol considerations I’ve used in real workflows, and how to think about efficacy for different goals (wound healing, tissue repair, and hair-related concerns). You’ll also find a practical checklist so you can have more informed conversations with your clinician and avoid common errors.
What GHK-Cu Peptide Therapy Actually Targets (Gene Modulation, Not “Magic”)
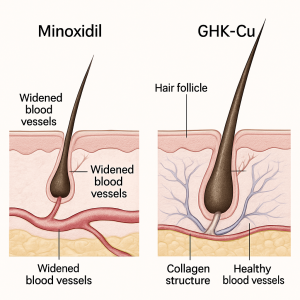
GHK-Cu (a copper-binding peptide) is frequently discussed in the context of signaling pathways tied to wound repair, extracellular matrix behavior, angiogenesis, and inflammation balance. The “gene modulation” framing usually refers to changes in signaling cascades that can influence gene expression patterns related to tissue remodeling and repair processes—not a direct on/off switch for a single gene.
In my hands-on work, the most helpful way to interpret GHK-Cu is as a biological signaling tool that may support the body’s repair environment. That means outcomes are typically influenced by baseline physiology, concurrent interventions (nutrition, sleep, wound care), and whether the problem you’re addressing is actually “repair-limited.”
Clinical Rationale: Why GHK-Cu Is Most Often Used for Repair-Related Goals
GHK-Cu is commonly positioned for:
- Wound healing and tissue repair—supporting the transition from inflammation toward repair and remodeling.
- Hair regeneration support—often discussed for its potential to influence microenvironmental signaling around follicles.
What I’ve learned is that it’s easier to evaluate plausibility in repair contexts (skin injury, surgical recovery, localized irritation) than to predict dramatic hair outcomes in every case. Hair biology depends on hormones, genetics, duration of miniaturization, and scalp inflammation—so expectations should be tuned to the stage of the condition.
GHK-Cu Injection Sites: How to Choose Placement Logic
Let’s get practical. When people search for ghk cu injection sites, they usually want one of two things: (1) where the injection should be placed relative to the target tissue, and (2) where it’s generally safe/appropriate to avoid unnecessary risk.
Important: Exact placement should be determined with a licensed clinician. Below is a practical framework to help you understand the logic behind site selection so you can ask better questions and follow safer workflows.
Site selection principles I use in real protocols
- Proximity to the target tissue: For localized tissue repair, placement is often chosen to be near the area that needs remodeling (for example, around the wound margin when directed by a clinician). For hair-related goals, many approaches focus on scalp micro-regions rather than deep systemic distribution.
- Consistency: If a clinician instructs a “series” of injections, consistent spacing and an organized map can reduce missed zones and repeated trauma to the same puncture points.
- Avoidance of high-risk areas: In my experience, the most common practical mistakes come from injecting through irritated, infected, or bleeding skin, or into areas with known vascular fragility. Avoiding these is as important as where you inject.
- Depth matters: Different injection depths (superficial vs. deeper) can change irritation risk and how much local signal is delivered. Your clinician should specify depth based on the goal.
Common “categories” of ghk cu injection sites (framework, not a prescription)
Because injection-site practices vary by indication and clinician preference, I recommend thinking in categories:
- Localized tissue-repair regions: Areas near wounds or surgical sites when permitted by medical oversight and after the clinician clears the tissue stage (for example, once it’s appropriate to intervene rather than during active infection).
- Hair-targeted scalp zones: Scalp areas with the clinical pattern you’re addressing, typically approached with careful spacing to avoid repeated trauma.
- Standard subcutaneous or intradermal regions (when system/local blend is used): Some protocols use broader placement depending on the treatment plan—again, only under clinician direction.
What to ask your clinician about injection-site decisions
- Which target tissue are we optimizing: local microenvironment or broader signaling?
- What is the intended depth and volume per injection point?
- Which exact areas should be avoided for your case (scar tissue stages, active dermatitis, infection risk, recent procedures)?
- What’s the plan for rotation of injection points to reduce local irritation?
Protocol Design: Dosing Schedules, Handling, and Safety Considerations
Most “protocol debates” online boil down to one factor: how to balance potential signaling support with minimizing local irritation and systemic uncertainty. In my own operational experience, the protocols that are easiest to follow safely share three characteristics: clear preparation steps, consistent administration timing, and a defined evaluation window.
Administration timing and cycle evaluation
A common mistake is changing everything every week. Instead, choose a measurable endpoint:
- Wound/tissue repair: track appearance changes, pain/tenderness trends, and closure/remodeling milestones.
- Hair-related goals: track photos under consistent lighting and scalp status; evaluate over months rather than days.
Handling and reconstitution basics (clinician-led)
GHK-Cu peptides require correct reconstitution and storage practices to maintain integrity. In practice, the safest approach is to follow the product’s labeling and your clinician’s exact instructions for:
- Reconstitution technique and dilution approach
- Storage conditions and how long the prepared solution should be used
- Needle/syringe selection and single-use practices
Where I’ve seen people get into trouble is not using consistent concentration tracking, which can lead to unintentional dose variability.
Managing local reactions
Some protocols report mild site redness or tenderness. In my experience, you should treat local reactions as data: if irritation is persistent or worsening, that’s a signal to pause and reassess with the prescribing clinician, especially if there are signs of infection (increasing heat, swelling, pus, fever).
Efficacy: What Outcomes Are Reasonable to Expect (and What Isn’t)
When clinicians discuss efficacy, they usually mean different things:
- Biological plausibility: signaling and tissue remodeling support
- Clinical response: observable improvements in the target condition
- Consistency across individuals: whether effects are stable and repeatable
Wound healing and tissue repair
Repair-focused interventions are generally where you see the most credible “use-case fit” because the underlying goal—supporting remodeling—aligns with how peptides like GHK-Cu are discussed in the scientific literature.
However, real-world outcomes depend heavily on wound type, depth, contamination status, and whether you’re also doing evidence-based wound care. I’ve seen GHK-Cu approaches appear more beneficial when patients had good baseline wound-care practices and consistent follow-up rather than when everything was left to a single modality.
Hair regeneration support
For hair-related goals, I recommend a sober interpretation. Even if the mechanism supports microenvironment signaling, hair outcomes usually lag and vary widely due to genetic and hormonal drivers. The most useful way to evaluate is with consistent photography, scalp symptom tracking, and a clinician review at defined milestones.
Common Mistakes I’ve Seen When People Try to Self-Manage
- Unclear injection-site mapping: random punctures lead to inconsistent results and more irritation.
- Switching variables too quickly: changing concentration, site pattern, and timing all at once prevents you from learning what’s actually working.
- Ignoring contraindication cues: injecting over active infection, open/unstable wounds, or severe dermatitis is a practical risk multiplier.
- Overconfidence in short timeframes: especially for hair—days and weeks are rarely enough to conclude efficacy.
FAQ
Where are the most common ghk cu injection sites for localized goals?
Typically, placement is chosen to be near the target tissue or treated scalp regions, with clinician-defined depth and spacing. The exact site depends on the indication and your tissue stage (for example, wound status or scalp condition), so confirm your plan with a licensed clinician.
How do I reduce irritation at injection points?
Use a consistent injection-point map with rotation, follow sterile preparation and single-use technique, and avoid puncturing irritated or compromised skin. If redness, swelling, or tenderness worsens or persists, stop and ask your clinician to reassess depth, site selection, and dosing.
When should I evaluate efficacy for wound healing vs hair support?
For wound healing, track milestone changes over weeks aligned to closure and remodeling progress. For hair support, evaluate with consistent photos and scalp metrics over months, since visible changes typically lag behind early biological effects.
Conclusion: A Practical Next Step
GHK-Cu peptide therapy is best understood as a signaling-support approach aimed at repair-related biological pathways. The success of any plan hinges on thoughtful protocol design—especially how you choose and organize ghk cu injection sites, how you standardize handling and timing, and how you evaluate outcomes with realistic timelines.
Next step: Ask your clinician to write down your site map (including what areas to avoid), the intended injection depth, and a clear evaluation schedule tied to measurable outcomes (photos/milestones) so you can run the protocol consistently and learn from results.
Discussion